Today's post is a guest post courtesy of my mom, Karen. She has a unique perspective based on her own help. Thanks for writing, Mama! Enjoy!
Several years ago someone
asked me what potentially life-threatening event I would find most frightening.
Without hesitation I said “Cancer.” Around that same time, someone else
asked me what I would do it I were ever diagnosed with cancer, to which I
replied I would probably shoot myself. Two of my dearest friends had recently
died of cancer and suffered mightily during their illness. The chemo and
radiation made them sick, and in the end they died anyway.
For most of my adult life
I’ve exercised and tried to eat healthily, assuming that this would help
protect me from physical ailments and diseases – including cancer.
Imagine my surprise, dismay, bewilderment, and sheer terror when in February
2014 I was diagnosed with breast cancer. It was stage 1B, survival rate greater
than 90%, but it was cancer and the survival rate wasn’t 100%. Did I shoot
myself? No, obviously not. Was this the scariest thing that had ever happened
to me during my 62 years on planet Earth? Yes, definitely. What could be
scarier? A few short months later I would find out.
On a sunny warm day in
April 2014, just over a month after my lumpectomy to remove my breast cancer,
my daughter Jennie called me while I was at work to ask if I could come over to
her house right away. She was very, very upset. I asked her what was wrong and
she wouldn’t tell me. I imagined all sorts of things that might be distressing
her so severely - cancer wasn’t on the list playing in my head. I grabbed my
keys and ran out of the office without even thinking to tell anyone where I was
going. Jennie is my only daughter, my first-born, and we’ve been incredibly
close from the moment of her birth. Luckily Jen lived only a couple of miles
from my office, and even more luckily – as much of a nervous wreck as I was – I
managed to speed to her house without crashing my car or getting stopped by the
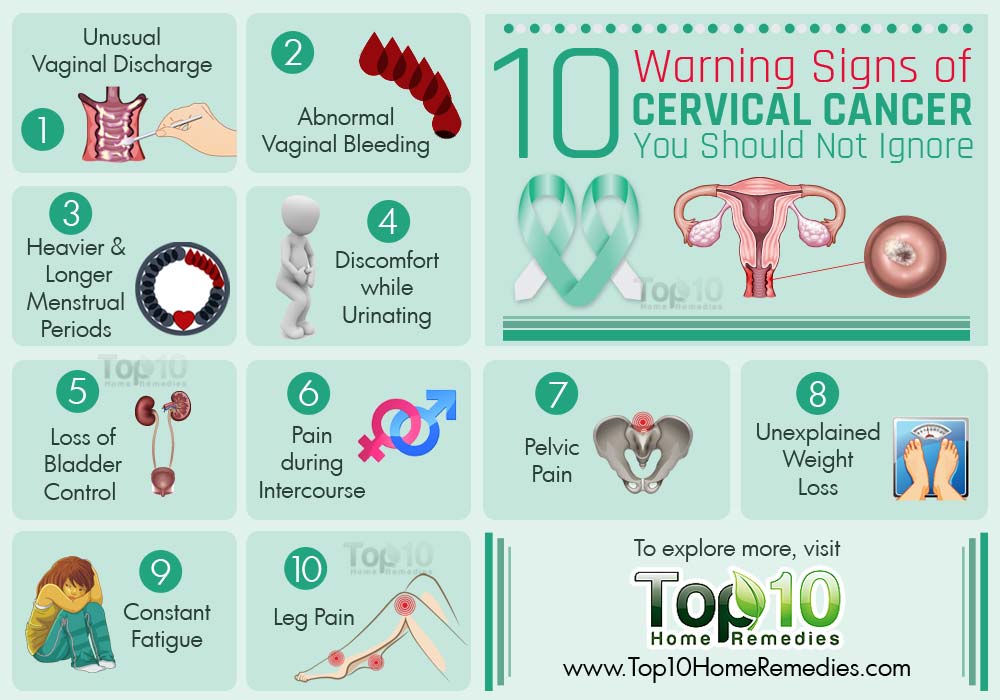
police. When I walked in the door, Jen told me she’d gotten the results of her
pap smear and that she had cervical cancer. She wouldn’t know the stage,
how bad it was, until she’d seen a gynecological oncologist. I felt like
the ground had suddenly dropped out from beneath my feet.
I wanted to scream, I
wanted to run, to disappear into thin air. This could not be happening. How
could this be?!?!? How could we both have cancer at the same time?!?!? What
were the odds? Probably a gazillion to one. This sounded much more deadly than
my breast cancer. Would my darling daughter, love of my life, die before me?
Could things somehow be reversed, could I take the death penalty in her
place? It was all I could do to hold it together while I was with her
that day. As scary as my cancer diagnosis had been, it paled in comparison to
hearing Jennie’s diagnosis. If there was ever a day I would have been
tempted to make a deal with the devil, that was the day. But luckily the
devil didn’t offer so instead, we just sat on the couch, holding each other and
crying together. We said over and over again how much we loved each other, and
that no matter what happened, we’d see it through together.
As it turned out, there was
a benefit to our having cancer at about the same time, particularly
emotionally. If only one of us had the disease, as caring and supportive as
either of us would have been for the other regardless, we had a much better
idea of what the other was going through, particularly emotionally. We
could understand on a gut level the anxiety, raw fear, depression, and even
anger the other was feeling without even having to say anything, without having
to ask, “What’s wrong?” We each understood when the other needed to be alone,
or needed to be with someone, even just sitting quietly reading together.
Luckily I had only a few very mild side-effects from my radiation treatments
and was able to go with Jen to doctor’s appointments, to the hospital when she
had her hysterectomy, and to stay at her house to help care for her
post-surgery.
The one thing I’m trying to
stop beating myself up about was not bugging Jennie to get regular
gynecological checkups. I would suggest it from time to time, she would
say she’d schedule one, but wouldn’t follow through. I had some idea of why
she wasn’t getting the exams and after all, she was an adult, so even though I
was concerned she was putting herself at risk for cancer, I bit my tongue
whenever I was tempted to nag her. I kept hoping that she’d go of her own
accord – which she eventually did, thank goodness! If I could have a
do-over on this, I think I’d be more of a nag – particularly knowing as I do
now how many relatively young women are stricken with cervical cancer, and how
critical it is to catch it as early as possible to maximize chance of survival.
As of a few weeks ago,
Jennie has been NED for 18 months – HURRAY!!! (Women who’ve survived
cancer say they are “NED” of that wonderful day when their oncologist tells
them they find “no evidence of disease”.) Am I still scared about whether
Jennie will be a long-time survivor of this dreadful disease? Yup, very
much so. It’s one of the few things that can wake me from a deep sleep and keep
me awake until dawn. But as time goes by and the number of Jen’s NED days
increases, the gut-wrenching fear occurs less and less often. Meanwhile, I’m
just profoundly grateful she finally went for a PAP smear when she did, for
each and every day she’s cancer free, for the wonderful times we share
together. And I’m extremely proud of her for all she’s doing to advocate for
better cervical cancer awareness and prevention education, and to provide
support to women who are battling this dreadful disease.
Oh – In case you’re wondering, as of
January 13, 2016 I’ve been NED for 20 months! Fingers crossed or prayers to the
deity of your choosing, Jen and I have many years left to enjoy sharing life’s
adventures together!